Cranial suture on the forehead of a child. Everything you need to know about the fontanel. What does he threaten?
The decisive role in the formation and subsequent development of the skull belongs to the brain, teeth, chewing muscles and sensory organs. During the process of growth, the head undergoes significant changes. During development, they appear age, gender and individual characteristics of the skull. Let's look at some of them.
Newborns
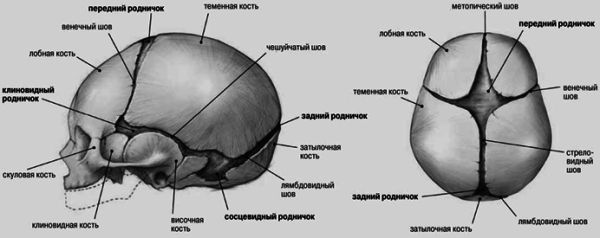
The baby's skull has a specific structure. The spaces between the bone elements are filled with connective tissue. Newborns are completely absent sutures of the skull. Anatomy This part of the body is of particular interest. At the junction of several bones there are 6 fontanelles. They are covered with connective tissue plates. There are two unpaired (posterior and anterior) and two paired (mastoid, sphenoid) fontanelles. The largest is considered to be the frontal one. It has a diamond shape. It is located at the convergence of the left and right frontal and both parietal bones. Due to the fontanelles it is very elastic. As the fetal head passes through the birth canal, the edges of the roof overlap each other in a tiled manner. Due to this, it decreases. By the age of two, as a rule, they have formed sutures of the skull. Anatomy previously studied in a rather original way. Medieval doctors applied hot iron to the fontanel area for diseases of the eyes and brain. After the formation of a scar, doctors caused suppuration with various irritants. So they believed that they were opening the way for accumulating harmful substances. In the configuration of the stitches, doctors tried to discern symbols and letters. Doctors believed that they contained information about the fate of the patient.

Features of the structure of the skull
This part of the body in a newborn is distinguished by the small size of the facial bones. Another specific feature is the fontanelles mentioned above. In the skull of a newborn there are traces of all 3 unfinished stages of ossification. The fontanelles are remnants of the membranous period. Their presence is of practical importance. They allow the roof bones to move. The anterior fontanel is located in the midline at the junction of 4 sutures: 2 halves of the coronary, frontal and sagittal. It becomes overgrown in the second year of life. The posterior fontanel has a triangular shape. It is located between the two in front and the scales of the occipital bone in the back. It grows over in the second month. The lateral fontanels are distinguished between sphenoid and mastoid. The first is located at the convergence of the parietal, frontal, temporal scales and greater wing of the sphenoid bones. Overgrows in the second or third month. The mastoid fontanel is located between the parietal bone, the base of the pyramid in the temporal and the occipital squama.

Cartilaginous stage
At this stage, the following age-related features of the skull are noted. Cartilaginous layers are found between the individual, unfused elements of the bones of the base. The air sinuses are not yet developed. Due to muscle weakness, various muscle ridges, tubercles and lines are poorly defined. For the same reason, also associated with the lack of chewing function, the jaws are underdeveloped. Hardly ever. The lower jaw consists of two unfused halves. Because of this, the face extends little forward relative to the skull. It is only 1/8. Moreover, in an adult the ratio of face to skull is 1/4.
Bone displacement
Skulls after birth are manifested in active expansion of the cavities - nasal, cerebral, oral and nasopharynx. This leads to a displacement of the bones surrounding them in the direction of the growth vectors. The movement is accompanied by an increase in length and thickness. With marginal and superficial growth, the curvature of the bones begins to change.

Postnatal period
At this stage, they manifest themselves in uneven growth of the facial and brain regions. The linear dimensions of the latter increase by 0.5, and the former by 3 times. The volume of the brain region doubles in the first six months, and by the 2nd year it triples. From the age of 7, growth slows down and accelerates again during puberty. By the age of 16-18, the development of the arch stops. The base increases in length up to 18-20 years and ends when the spheno-occipital synchondrosis closes. The growth of the facial region is longer and more uniform. The bones around the mouth grow most actively. Age features of the skull in the process of growth, they manifest themselves in the fusion of parts of bones separated in newborns, differentiation in structure, and pneumatization. The relief of the internal and external surfaces becomes more defined. At an early age, smooth edges form on the seams; by the age of 20, jagged joints form.

Final stages
By the age of forty, obliteration of the sutures begins. It covers all or most connections. In old and senile age, osteoporosis of the cranial bones is observed. The thinning of the plates of the compact substance begins. In some cases, thickening of the bones is observed. Atrophy in the jaws becomes more pronounced in the facial region due to tooth loss. This causes an increase in the angle of the lower jaw. As a result, the chin comes forward.
Gender characteristics
There are several criteria by which a male skull differs from a female one. Such signs include the degree of severity of roughness and tubercles in the areas of muscle attachment, development of the occipital outer protuberance, protrusion of the upper jaw, etc. The male skull is more developed in comparison with the female. Its outlines are more angular due to the severity of roughness and tuberosity in the areas of attachment of the masticatory, temporal, occipital and cervical muscles. The frontal and parietal tubercles are more developed in women, while in men the glabella and brow ridges are more developed. the latter have a heavier and larger lower jaw. In the area of the lower edge and corners of the inner part of the chin, tuberosity is clearly expressed. This is caused by the attachment of the digastric, masticatory and pterygoid muscles. Depending on gender, the shape of the human skull also differs. Men have a sloping forehead, which turns into a rounded crown. An elevation is often observed in the direction of the sagittal suture. Women's foreheads are more vertical. It turns into a flat crown. Men have lower eye sockets. As a rule, they have a rectangular shape. Their upper edge is thickened. In women, the eye sockets are located higher. They are close to oval or round in shape with sharper and thinner upper edges. On the female skull, the alveolar process often protrudes forward. The nasofrontal angle in men is clearly expressed in most cases. On the female skull, the frontal bone transitions more smoothly to the nasal bones.

Additionally
The shape of a person's skull does not affect mental abilities. Based on the results of numerous studies by anthropologists, it can be concluded that there is no reason to believe that the size of the brain region predominates in any race. The Bushmen, Pygmies and some other tribes have slightly smaller heads than other people. This is due to their small stature. Often, a decrease in head size can be the result of poor nutrition over the centuries and the influence of other unfavorable factors.
Craniosynostosis is characterized by premature fusion of one or more cranial sutures, often resulting in an abnormal head shape. This may be the result of primary abnormal ossification (primary craniosynostosis) or, more commonly, a growth disorder of the brain (secondary craniosynostosis).
The disease often occurs in utero or at a very early age. It can only be treated surgically, although a positive outcome is not possible in all cases.
Classification of craniosynostosis and causes of its development
Normal ossification of the cranial vault begins in the central region of each bone of the skull and extends outward to the cranial sutures. What indicates normal?
- When the coronal suture separates the two frontal bones from the parietal bones.
- The metopic suture separates the frontal bones.
- The sagittal suture separates the two parietal bones.
- The lambdoid suture separates the occipital bone from the two parietal bones.
The main factor that inhibits untimely fusion of the skull bones is the continued growth of the brain. It is worth emphasizing that the normal growth of each cranial bone occurs perpendicular to each suture.
- Simple craniosynostosis is the term used in situations where only one suture fuses prematurely.
- The term complex or junctional craniosynostosis is used to describe the premature fusion of multiple sutures.
- When children showing symptoms of craniosynostosis also suffer from other body deformities, it is called syndromic craniosynostosis.
Primary craniosynostosis
If one or more sutures undergo premature fusion, skull growth may be limited by the perpendicular sutures. If multiple sutures are fused while the brain is still changing in size, intracranial pressure may increase. And this often ends in a number of complex symptoms, even death.
Types of primary craniosynostosis (premature fusion)
- Scaphocephaly is a sagittal suture.
- Anterior plagiocephaly is the first coronal suture.
- Brachycephaly is a bilateral coronal suture.
- Posterior plagiocephaly is early closure of one lambdoid suture.
- Trigonocephaly is premature fusion of the metopic suture.
Secondary craniosynostosis
More often than with the primary type, this type of pathology can lead to early fusion of the sutures due to primary failure of brain growth. Since the growth of the brain controls the distance of the bone plates from each other, a disorder of its growth is the main reason for the premature fusion of all sutures.
With this type of pathology, intracranial pressure is usually normal, and there is rarely a need for surgery. Typically, lack of brain growth leads to microcephaly. Premature closure of the suture, which does not pose a threat to brain growth, also does not require surgical intervention.
Intrauterine spatial restrictions may play a role in premature fusion of the fetal skull sutures. This has been demonstrated in cases of coronal craniosynostosis. Other secondary causes include systemic disorders affecting bone metabolism such as rickets and hypercalcemia.
Causes and consequences of early craniosynostosis
Several theories have been proposed for the etiology of primary craniosynostosis. But the most widespread option is the one with the etiology of a primary defect in the mesenchymal layers of the bones of the skull.
Secondary craniosynostosis usually develops along with systemic disorders
- These are endocrine disorders (hyperthyroidism, hypophosphatemia, vitamin D deficiency, renal osteodystrophy, hypercalcemia and rickets).
- Hematological diseases that cause bone marrow hyperplasia, for example, sickle cell disease, thalassemia.
- Low rates of brain growth, including microcephaly and its underlying causes, such as hydrocephalus.

The causes of syndromic craniosynostosis are genetic mutations responsible for fibroblast growth factor receptors of the second and third classes.
Other important factors to consider when studying the etiology of the disease
- Differentiating plagiocephaly, which is often the result of positional fusion (which does not require surgery and is quite common) from lambdoid suture fusion, is an extremely important aspect.
- The presence of multiple adhesions is suggestive of a craniofacial syndrome, which often requires diagnostic evaluation in pediatric genetics.
Symptoms of craniosynostosis and diagnostic methods
Craniosynostosis in all cases is characterized by an irregular shape of the skull, which in a child is determined by the type of craniosynostosis.
Main features
- A rigid bone ridge, easily palpable along the pathological suture.
- The soft spot (fontanelle) disappears, the child's head changes shape, and sensitivity in these areas is usually altered.
- The baby's head does not grow in proportion to the rest of the body.
- Increased intracranial pressure.
In some cases, craniosynostosis may not be noticeable until several months after birth.
Increased intracranial pressure is a common feature of all types of craniosynostosis, with the exception of some secondary pathologies. When only one suture fuses prematurely, increased intracranial pressure occurs in less than 15% of children. However, in syndromic craniosynostosis, where multiple sutures are involved, increased pressure can be observed in 60% of cases.
If a child suffers from a mild form of craniosynostosis, the disease may not be noticed until patients begin to experience problems due to increased intracranial pressure. This usually occurs between the ages of four and eight years.
Symptoms of increased intracranial pressure
- They begin with persistent headaches, usually worse in the morning and at night.
- Problems with vision - double vision, blurred vision or impaired color vision.
- Unexplained decline in the child's mental abilities.
If your child complains of any of the above symptoms, you should contact your pediatrician as soon as possible. In most cases, these symptoms will not be caused by increased intracranial pressure, but they should definitely be investigated.
If left untreated, other symptoms of increased intracranial pressure may include:
- vomiting;
- irritability;
- lethargy and lack of response;
- swollen eyes or difficulty seeing a moving object.
- hearing impairment;
- labored breathing.
Upon closer examination of the skull, it becomes clear that its shape does not always confirm the diagnosis of craniosynostosis. In such cases, a number of visual examination methods are used, for example, a skull x-ray.
X-rays are performed in several projections - anterior, posterior, lateral and superior. Prematurely fused sutures are easily identified by the absence of connected lines and the presence of bone ridges along the suture line. The sutures themselves are either not visible, or their location shows evidence of sclerosis.
A 3D cranial CT scan is usually not needed for most infants. The technique is sometimes performed when surgery is being considered as the next step in treatment or when X-ray results are equivocal.
Pathology correction methods, possible complications and consequences

Over the past 30 years, modern medicine has developed a greater understanding of the pathophysiology and treatment of craniosynostosis. Currently, surgery generally remains the main type of treatment for the correction of cranial deformities in children with fusions of 1-2 sutures, resulting in a malformed head. For children with microcephaly, which is often seen with mild craniosynostosis, surgery is usually not required.
When drawing up a therapeutic regimen, specialists must take into account a number of points.
- Patients with microcephaly should have the cause of this disease has been studied.
- When you first contact head circumference is measured in the longitudinal direction and further changes are monitored. The doctor should verify normal brain growth in patients with primary craniosynostosis.
- Should be carried out regularly monitoring for signs and symptoms of increased intracranial pressure.
- If there is a suspicion of increased intracranial pressure, then it is very appropriate neurosurgical consultation.
- To preserve visual function in patients with increased intracranial pressure, it is necessary to carry out additional ophthalmological consultations.
Surgery is usually planned for elevated intracranial pressure or to correct cranial deformity. The operation is usually performed in the first year of life.
Conditions for surgery
- If the shape of the head does not change for the better at the age of two months, then the anomaly is unlikely to change with age. Early intervention is indicated if children may be candidates for minimally invasive surgery. It is worth noting that the deformity is more noticeable in the thoracic period, and it may become less obvious with age.
- As the child grows and develops more hair, the visible signs of the abnormality may decrease.
- Indications for surgical correction of craniosynostosis depend on the age, general condition of the child and the number of prematurely fused sutures.
- Surgical treatment of cranial or craniofacial deformity is performed in children aged 3–6 months, although approaches vary among surgeons.

Surgery in infants can result in relatively large losses of blood volume. Accordingly, minimally invasive surgical techniques should be considered. One promising option is the use of intraoperative tranexamic acid. Patients with indications for surgical correction of craniosynostosis were pretreated with erythropoietin and tranexamic acid, which allowed them to maintain lower amounts of blood loss.
Other features of surgery
- Surgery in infants over 8 months of age may be associated with slower skull growth.
- Infants diagnosed with syndromic craniosynostosis should have surgery as soon as possible.
- The results of the operation are better if it is performed on infants under 6 months of age.
Craniostenosis - (from the Greek kranion - skull and stenosis - narrowing) premature closure of cranial sutures or their congenital absence.
The baby's skull consists of 6 skull bones: the frontal bone, the occipital bone, two parietal bones, two temporal bones. Normally, all these bones of the skull are not fused, the anterior and posterior fontanelles are open. The bones listed above are held together by strong, elastic tissues called sutures. Without the flexibility of these sutures, a child's brain cannot grow properly. The brain grows and the lid of the child's skull should also expand. The sutures respond to brain growth by "stretching" and "producing" new bone, thereby allowing the skull to grow along with the brain. Normal growth of the skull occurs perpendicular to each suture.
The posterior fontanelle closes by the end of the 2nd month, the anterior one - during the 2nd year of life. By the end of the 6th month of life, the bones of the cranial vault are connected to each other by a dense fibrous membrane. By the end of the 1st year of life, the child’s head size is 90%, and by 6 years it reaches 95% of the adult’s head size. The closure of the sutures by connecting the jagged edges of the bones begins by the end of the 1st year of life and is completely completed by the age of 12-14 years.
Premature and uneven overgrowth of fontanelles and cranial sutures in children - craniostenosis - interferes with normal brain development and leads to the creation of conditions for liquor-dynamic disorders. Liquorodynamic disorders are usually called pathological conditions in which the secretion, resorption and circulation of cerebrospinal fluid are impaired. The incidence of craniostenosis is 1 in 1000 newborns. With craniostenosis, intracranial pressure is usually increased, which is why hypertensive headache is characteristic, and congestive optic discs may develop, followed by secondary atrophy and visual impairment, and mental retardation.
Causes
There are primary (idiopathic) and secondary craniosynostosis. The development of secondary craniosynostosis can be due to various reasons. These may include vitamin D deficiency rickets, hypophosphatemia, and overdose of thyroid hormone in cases of treatment of congenital hypothyroid oligophrenia (cretinism).
What's happening?
The healing of the sutures of the skull is not only premature, but also uneven and usually leads to deformation of the skull. In the process of monitoring the development of the shape of the brain skull, the so-called cranial index (CI) is taken into account - the ratio of the transverse size of the skull to its longitudinal size, multiplied by 100. With a normal (average) ratio of the transverse and longitudinal dimensions of the head (with mesocephaly), the cranial index in men is 76-80.9, for women - 77-81.9.
With premature overgrowth of the sagittal suture (sagittal synostosis), dolichocephaly, in which the skull increases in the anteroposterior direction and is reduced in transverse size. In such cases, the head turns out to be narrow and elongated. CHI is less than 75.
 A variant of dolichocephaly caused by premature fusion of the sagittal suture, in which there is a restriction in the growth of the skull in the transverse direction and excessive growth in length, may be scaphocephaly(from the Greek skaphe - boat), cymbocephaly (scaphoid head, keel head), in which a long narrow head is formed with a protruding forehead and back of the head, reminiscent of a boat turned upside down with its keel. A skull that is elongated in the longitudinal direction with a depression in the parietal region is called saddle-shaped.
A variant of dolichocephaly caused by premature fusion of the sagittal suture, in which there is a restriction in the growth of the skull in the transverse direction and excessive growth in length, may be scaphocephaly(from the Greek skaphe - boat), cymbocephaly (scaphoid head, keel head), in which a long narrow head is formed with a protruding forehead and back of the head, reminiscent of a boat turned upside down with its keel. A skull that is elongated in the longitudinal direction with a depression in the parietal region is called saddle-shaped.
A variant of skull deformation, in which the skull has an increased transverse size due to premature fusion of the coronal (coronal) sutures (coronal, or coronal, synostosis), is brachycephaly(from the Greek brachis - short and kephale - head), the head is wide and shortened, the cranial index is over 81. With brachycephaly, due to bilateral coronary synostosis, the face is flattened, exophthalmos is often manifested - anterior displacement of one or both eyeballs.
With premature fusion of the coronary suture on one side, plagiocephaly, or cross-headedness (from the Greek plagios - oblique and kephale - head). In such cases, the skull is asymmetrical, the frontal bone on the side of the synostosis is flattened, and exophthalmos and enlargement of the middle and posterior cranial fossae are possible on the same side.
 If premature combined fusion of the coronal and sagittal cranial sutures occurs, the growth of the skull occurs mainly towards the anterior fontanelle and base, which leads to an increase in the height of the head while limiting its growth in the longitudinal and transverse directions. As a result, a tall, conical skull is formed, somewhat flattened in the anteroposterior direction (acrocrania); it is often called a tower skull. A variant of the tower skull is oxycephaly, or pointed head (from the Greek oxys - sharp, kephale - head), in which early fusion of the cranial sutures leads to the formation of a high, tapering upward skull with a forehead sloping back.
If premature combined fusion of the coronal and sagittal cranial sutures occurs, the growth of the skull occurs mainly towards the anterior fontanelle and base, which leads to an increase in the height of the head while limiting its growth in the longitudinal and transverse directions. As a result, a tall, conical skull is formed, somewhat flattened in the anteroposterior direction (acrocrania); it is often called a tower skull. A variant of the tower skull is oxycephaly, or pointed head (from the Greek oxys - sharp, kephale - head), in which early fusion of the cranial sutures leads to the formation of a high, tapering upward skull with a forehead sloping back.
A variant of skull deformation, characterized by a narrow frontal and broad occipital bones, is formed due to premature fusion of the frontal suture. In this case, the frontal bones grow together at an angle (normally, the frontal suture heals only at the end of the 2nd year of life) and a “ridge” is formed at the site of the frontal suture. If in such cases the posterior parts of the skull enlarge compensatoryly and its base deepens, trigonocrania, or a triangular skull, occurs (from the Greek trigonon - triangle, kephale - head).
Isolated synostosis of the lambdoid suture is extremely rare and is accompanied by flattening of the occiput and compensatory expansion of the anterior part of the skull with an enlargement of the anterior fontanel. It is often combined with premature closure of the sagittal suture.
At secondary craniostenosis at an early stage of its development, conservative treatment of the underlying disease can be effective. In case of primary craniostenosis, as well as in case of secondary craniostenosis in the case of already developed significant intracranial hypertension, decompressive surgery is indicated: the formation of craniectomy passages up to 1 cm wide along the line of suture ossifications. Timely surgical treatment for craniostenosis can ensure further normal brain development.
Treatment
The most active period of brain growth is considered to be up to two years of age. Thus, from a functional point of view, craniostenosis can be prevented by early surgical treatment. The optimal age for surgery for craniosynostosis can be considered the period from 3 to 9 months. The advantages of treatment at this age include: ease of manipulation with the thin and soft bones of the skull; facilitating the final remodeling of the skull shape by the rapidly growing brain; more complete and rapid healing of residual bone defects.
If treatment is performed after age five, it is doubtful that it will lead to significant improvement in brain function. To a greater extent, the operation will be aimed at eliminating the deformation of the head. The main feature of modern surgical treatment is not only an increase in the volume of the skull, but also correction of its shape and associated facial deformation during one operation.
What parents should pay attention to
- Unusual shape of a child's head
- Early closure of a large fontanel (up to a year)
- The growth rate of the child’s head circumference does not correspond to the age norm (see the head circumference of boys and the head circumference of girls)
- Poor sleep, restlessness of the child, deterioration of the child when the weather changes, regurgitation, lag in psychomotor development (see psychomotor development of the child)
If the above symptoms are detected in a child, you should contact a specialist:
- Neuropathologist – assesses the presence of neurological symptoms and delayed development of the child
- Ophthalmologist - assesses signs of intracranial hypertension based on the results of fundus examination (in advanced cases - decreased visual acuity)
- Pediatrician – assesses the presence of other anomalies in the development of organs and systems, somatic pathology
- Genetics – reveals the presence of the genetic nature of the disease, the likelihood of anomalies in other organs and systems and the prognosis of the recurrence of a similar pathology in the next child
Please note that it is better to play it safe and refer a child with a skull deformation to a specialist than to miss the pathology.
Did you like the article? Share the link
The skull of a newborn baby consists of six separate bones connected by thin, elastic layers of fibrous tissue. In medical practice they are called cranial sutures or fontanelles.
Such areas are necessary so that the bones partially overlap during the birth process. This nuance allows rule out brain injury newborn
The fontanelles disappear in the child during the first year of life. Premature fusion of soft tissues is called craniosynostosis (craniostenosis) and is a serious pathology.
Concept and characteristics
Craniostenosis in a child - photo:
Craniosynostosis is a pathology in which early closure or complete absence of cranial sutures occurs in children. This condition leads to intracranial hypertension, significant deformation of the skull and limitation of its volume.
Pathology can be primary or secondary. In the first case, the disease develops against the background of improper formation of the bone skeleton and ossification of the skull; in the second, disruption of the process of brain growth plays an important role.
Features of the disease:
- pathology begins to progress at the stage of intrauterine development of the fetus;
- in rare cases, the disease manifests itself in newborns in the first months of life;
- if the pathology was not detected at birth or in the first months of life, then at an older age the risk of its development is excluded.
Causes
The basis of the pathological process is a violation of the formation of the fetal bone skeleton.
Reasons for the development of this condition in medical practice not fully studied, but experts identify several factors that increase the risk of craniosynostosis in newborns.

In most cases, the pathology is combined with other defects in the development of the child.
Causes of pathology are the following factors:
- hereditary pathologies (for example, Crouzon syndrome);
- consequences of hormonal imbalance;
- serious endocrine pathologies;
- the position of the fetus in which its skull is compressed by the uterus;
- premature synostosis of one or more cranial sutures;
- abuse of bad habits during pregnancy;
- uncontrolled use of potent medications during gestation;
- abnormal position of the fetus during pregnancy;
- slow brain growth;
- perinatal trauma;
- hematological diseases;
- genetic abnormalities;
- exposure to intrauterine infections.
What are the signs of Down syndrome in a newborn? find out right now.
Classification: types and forms
In medical practice, the classification of craniosynostosis is carried out in several directions. The pathology may be syndromic and non-syndromic. In the first case, the disease is accompanied by other defects, in the second it develops independently.

Depending on the number of fused sutures, craniosynostosis is divided into pansynostosis(fusion of all sutures of the skull), monosynostosis(splicing one seam) and polysynostosis(merging several seams).
Monosynostosis is divided into separate types:
- lambdoid unilateral or bilateral craniosynostosis (premature fusion of the lambdoid suture);
- isolatedmetopic craniosynostosis (overgrowth of the metopic suture);
- coronary unilateral or bilateral craniosynostosis (fusion of the coronal suture);
- isolated sagittal Craniosynostosis (premature fusion of the sagittal suture).
Symptoms and signs
The symptoms of craniosynostosis directly depend on the stage of progression of the pathological process and the number of closed sutures. The period of fetal formation during which this pathology manifests itself plays an important role.
If the sutures begin to close in the first months of pregnancy, the symptoms will be more pronounced.
External signs of craniosynostosis appear immediately after the birth of the child and clearly visible visually.
Symptoms pathology are the following factors:

Diagnostics
Diagnosis of craniosynostosis in a child begins with a visual examination. The doctor palpates the fontanelles, detects deviations from the norm and collects a complete medical history. The parameters of the baby's skull are measured using special tape.
Based on the collected data, the specialist prescribes additional tests, procedures and consultations with specialized doctors. The examination of the newborn should be carried out comprehensively and include identification of possible additional pathologies.
Diagnostics Craniosynostosis includes the following procedures:
- MRI and CT of the brain;
- angiography;
- neurological examination;
- physical examination;
- Doppler ultrasound of the vessels of the neck and head;
- neurosonography;
- consultation with an ophthalmologist;
- ophthalmoscopy;
- X-ray of the brain.
Treatment methods

When treating craniosynostosis in medical practice, two main methods are used - surgery and endoscopy.
Radical ways to correct the disease are the most effective.
Endoscopy is carried out only until the child is six months old and in the presence of minimal complications of the pathological process. The decision to use a specific treatment method for craniosynostosis is made by the doctor based on a comprehensive examination of the baby.
Therapeutic regimen
Therapeutic treatment of craniosynostosis includes several stages. After examining the child, the doctor determines the degree of development of the disease and identifies the presence of complications of the pathological process.
There are certain contraindications for surgical intervention.
For example, a period of exacerbation of a viral disease, diseases associated with the composition of the blood, or the baby has a high fever. After the examination a specific type of surgical intervention is selected.
Treatment regimen for craniosynostosis:

Surgical
Surgical intervention is the main and most effective way elimination of craniosynostosis.
The purpose of this procedure is to give the skull the correct shape by cutting prematurely fused sutures.
In some cases, specialists use distraction devices to remodel bones.
Features of the operation:
- It is recommended to carry out the procedure for up to seven months (active brain growth occurs in the first year of a child’s life).
- Early surgical intervention allows for increased regression of all existing pathological conditions in the child.
- A timely operation significantly increases the likelihood of a favorable prognosis for the baby.
You will find information on the treatment of hydrocephalus in a child on our website.
Forecasts
Craniosynostosis in children - before and after photos:

Prognosis for craniosynostosis depends on the form of the disease present. Almost completely eliminate the consequences the disease can only be treated in a timely manner.
In some cases, complications lead to the death of the child in the first year of life.
Children first become infected with ARVI, and then, against the background of a cold, they develop pneumonia. Poor prognosis observed only in the syndromic form of craniosynostosis.
Nuances prognosis for pathology:
- The earlier surgery is performed, the lower the risk of complications.
- Endoscopy is accompanied by less blood loss for the child (the procedure has age restrictions).
- If the operation is performed after the child reaches three years of age, the risk of complications will be maximum.
Specific measures to prevent craniosynostosis in children does not exist.
Non-specific preventive actions include a woman’s attentive attitude to her own health and the period of pregnancy, regular examinations by a gynecologist, as well as timely prevention of the risk of developing intrauterine infections.
If a child is diagnosed with craniosynostosis, then treatment of the disease is necessary. carry out as soon as possible.
You can learn about the prognosis for craniosynostosis in children from the video:
We kindly ask you not to self-medicate. Make an appointment with a doctor!
Craniosynostosis is a pathology of healing of the sutures of the skull, which causes deformation of the normal shape of the head. Metopic synostosis (trigonocephaly) is the rarest type of craniosynostosis, accounting for about 10-25% of such diseases.
Metopic synostosis in a child is usually diagnosed in the maternity hospital. Mild forms can be detected during examination by a neonatologist or pediatrician (at a later age). Trigonocephaly is treated with surgery.
Metopic synostosis occurs as a result of premature fusion of the skull in the area of the metopic suture. This anatomical structure connects the parts of the frontal bone. It is considered normal for the metopic suture to close within 8-24 months. Untimely closure of the seam causes deformation of the skull, as well as the upper part of the face.
There are two types of metopic synostosis: trigonocephaly and asymptomatic craniosynostosis. The first type of deformation has the following features:
- Suture closure usually occurs in utero or in early childhood (up to 2 months);
- The deformity is formed according to the type of hypotelorism or trigonocephaly;
- Clinically, this is manifested by a decrease in the distance between the orbits;
- The location of the overgrowth can be determined by palpation in the form of a small hump;
- Complete growth and smoothing takes up to 2 months.
Early closure of the metopic suture causes insufficient development of the frontal bone. Visually, this is characterized as a disproportionate, yet relatively small oval face.
Type 2 (asymptomatic)  Craniosynostosis) develops relatively later. The healing of the mepotic suture is observed at the age of 3-4 months. A bone ridge is formed at the junction, which can be detected by palpation. Asymptomatic craniosynostosis does not deform the frontal bone and facial oval, so visual diagnosis is difficult.
Craniosynostosis) develops relatively later. The healing of the mepotic suture is observed at the age of 3-4 months. A bone ridge is formed at the junction, which can be detected by palpation. Asymptomatic craniosynostosis does not deform the frontal bone and facial oval, so visual diagnosis is difficult.
General characteristics of the disease
Metopic synostosis in a child is a relatively rare pathology of this group of diseases. In recent years, there has been a trend towards an increase in the incidence of the disease in the population due to the increased influence of teratogenic factors during pregnancy (radiation, drugs, unhealthy diet). The trigger for the development of the disease can be a skull injury during the passage of the child through the birth canal.
The clinical picture of metopic synostosis is characterized by:
- Hypertension syndrome;
- Mental disorders;
- Pathology of the optic nerve.
Hypertension is caused by increased pressure inside the skull. Due to the pathological narrowing of the space, blood vessels do not have the opportunity to develop as usual. This can cause disruption of local circulation with subsequent ischemia.

The most active growth of the main brain and neurons occurs in the period up to two years. Premature closure of the metopic suture causes a lack of space for the growth of gray matter, so trigonocephaly leads to mental disability. At an early age, the developmental pathology of this area is reversible. It is corrected through surgery.
Reducing the distance between the orbits contributes to compression of the optic nerve. Pulses passing through such beams are distorted, which leads to the occurrence of ophthalmic pathologies.
The diagnosis of metopic synostosis can be made by a pediatrician during a routine examination of the child. In addition to the characteristic shape of the face, when palpating the area of the overgrown suture, a ridge of inert origin can be detected. Neurological symptoms of trigonocephaly are difficult to determine, so diagnosis is based on checking reflexes during examination by a neurologist.
Computed tomography is used to carry out differential diagnosis. The method makes it possible to verify the presence of disproportions in the craniocerebral region, as well as to confirm the presence of compression of the frontal parts of the brain in the sagittal direction.
Treatment of metopic synostosis
Trigonocephaly is an indication for surgery.

Timely diagnosis and immediate treatment reduces the risk of complications to a minimum. The optimal period for surgical intervention is considered to be between 3 and 9 months of age. Bone structures during this period are relatively labile, so the operation is not complicated by the need for craniotomy.
The rapid growth of the brain during this period contributes to the rapid equalization of deformation without consequences for the nervous system. Indirect defects heal completely, leaving almost no scars, and the rehabilitation period is relatively better.
A feature of surgical intervention for metopic synostosis is an increase in the volume of the cranium along with a change in its shape. This eliminates the deformation of the facial region. The regenerative abilities of the nervous system depend on age.
The easier the patient's condition, the fewer complications there will be after surgery. Surgical intervention after 5 years is not very effective. This operation will not improve cognitive functions.
Without surgery, trigonocephaly will progress over time. Deep deformation of the skull without the necessary plastic surgery can cause complete mental incapacity and deterioration of vision. After surgical intervention during rehabilitation, the use of physiotherapeutic procedures is recommended.
Metopic synostosis is a severe form of deformation of the skull in the sagittal direction. This pathology can cause a number of complications. Timely diagnosis of the disease plays an important role.

After detecting suspicious symptoms, you must inform your pediatrician or contact a neurologist yourself. It must be remembered that the earlier surgery is performed, the fewer consequences there will be in the future.









